Long COVID & ME/CFS — clear, in small steps
You don't have to read everything at once. Pick what matters most today — calm, vetted orientation without information pressure. Not a diagnosis, not a promise of a cure.
The essentials in 5 points
You don't have to read everything at once. These five points are enough to start.
→ No. A biological orientation — not a diagnosis, not a treatment.
→ A biological orientation map: which mechanisms may be more prominent in your case.
→ A short medical teleconsult → saliva sample at home → your report.
→ €599 one-time, instalments possible.
→ PEM: do not push through. Pacing first, respect your limits.
What do you need right now?
Acute or severe symptoms (e.g. new severe chest pain, severe shortness of breath, loss of consciousness)? Call emergency services (112) immediately.
In 60 seconds
The basics — each in a few calm sentences.
After a COVID-19 infection most people recover. In some, symptoms persist or newly appear — this is often called Long COVID. Symptoms vary widely: severe exhaustion, trouble concentrating, dizziness, palpitations, sleep problems or a marked worsening after exertion. There is probably no single cause — several processes in the body can interact.
The report compares patterns in your DNA with patterns observed more often in research groups with Long COVID. This can help you understand possible links. But it does not prove what causes a single symptom, is not a diagnosis and does not replace medical advice.
For complex conditions, looking for a single gene often isn't enough. PrecisionLife research therefore examines combinations of genetic variants. Such recurring patterns are called genetic signatures. For individuals they are not proof of a cause and not an automatic treatment recommendation.
PEM means: symptoms worsen markedly after physical, cognitive, emotional or sensory exertion. This can happen with a delay, e.g. only the next day. Such a crash is not the same as normal tiredness. If you recognise this pattern, it makes sense to take your limits seriously and discuss it medically.
Long COVID is an umbrella term for longer-lasting symptoms after a COVID-19 infection. Some people develop a condition that resembles ME/CFS or meets its criteria. PEM is especially important here. Not every fatigue is ME/CFS, and not every person with Long COVID has ME/CFS.
- 1.Long COVID is real and can affect several body systems.
- 2.Long COVID does not look the same in everyone.
- 3.Several factors and mechanisms can play a role at the same time.
- 4.PEM is more than normal exhaustion and should be taken seriously.
- 5.Genetic patterns give hints and context — not a diagnosis, not automatic therapy.
- 6.Research on subgroups may enable better care in the future, but is not yet a personal recommendation.
Why not one gene?
Long COVID does not arise from a single 'switch'. Many small genetic contributions together form a pattern – like a recipe, not a single ingredient. PrecisionLife's combinatorial analysis detects exactly these combinations, where classic single-gene studies see nothing.
How many genes become one pattern
It is not a single gene that decides. Many small variants form, in combination, a recurring pattern — the genetic signature PrecisionLife detects.
Schematic. A research signal, not an individual diagnosis.
Research status: a combinatorial ME/CFS analysis (DecodeME cohort, PrecisionLife; preprint 2026) identified 259 ME-associated core genes; 76 of 180 genes previously linked to Long COVID were also significant in the ME analysis — overlapping yet distinct biology of both conditions. A research signal, not an individual diagnosis (preprint, not yet peer-reviewed).
Six mechanisms — in detail
The report treats these six areas as possible levels of explanation — not as a complete list of all causes, and not as a proven cause in you. Tap a card.
When the immune response gets out of balance

Immune response
Your immune system detects and fights infections. In Long COVID it often stays 'switched on': inflammatory signals keep running while the defence cells become exhausted.
What does this mean for me? Explains a persistent feeling of illness, susceptibility to infections and flare-ups.
Related symptoms: Fatigue · flare-ups · flu-like feeling
When cells provide energy less well
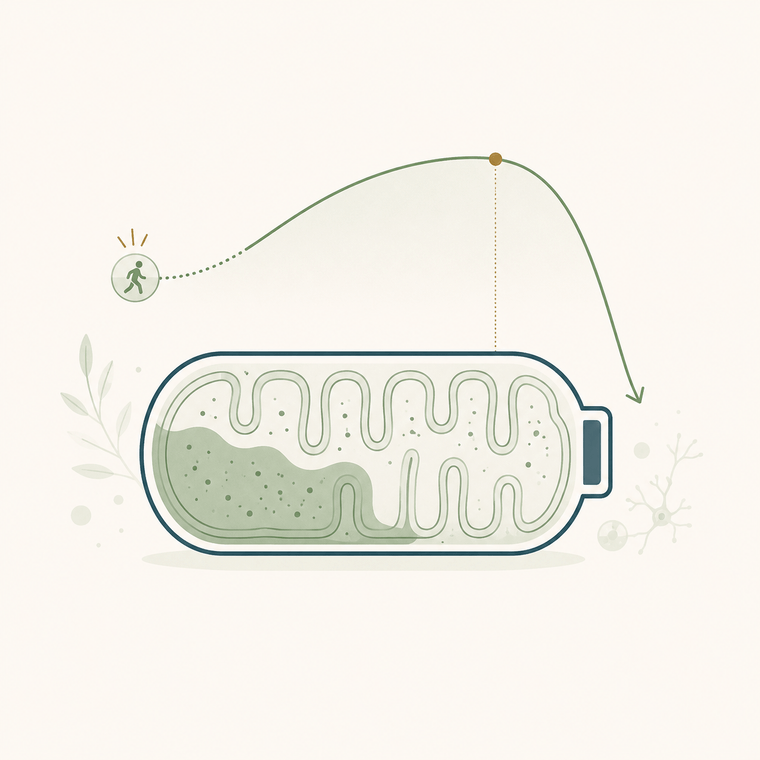
Cellular energy
The mitochondria are the power plants of your cells. If they work more slowly after the infection, your body has a lower 'energy ceiling' – small activities can lead to a crash hours to days later.
What does this mean for me? Explains Post-Exertional Malaise (PEM) and exertion intolerance.
Related symptoms: PEM · fatigue · post-exertional crash
When thinking and concentration become harder
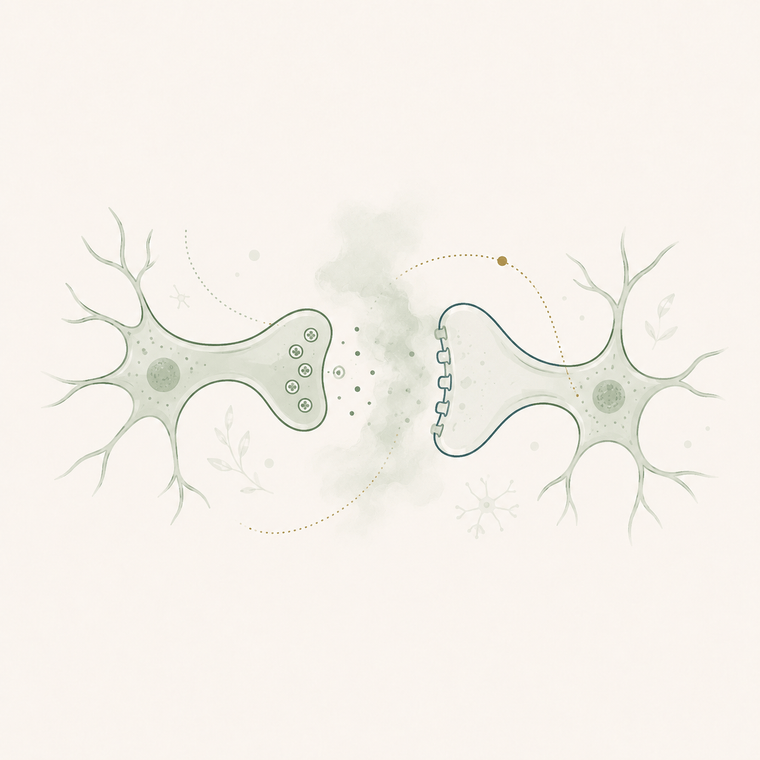
Cognition / 'Brain Fog'
Inflammation, altered blood flow and less energy in the brain can impair concentration, memory and word-finding.
What does this mean for me? Explains the feeling of not being able to 'think clearly'.
Related symptoms: Brain Fog · word-finding · concentration
When circulation and blood vessels may be involved
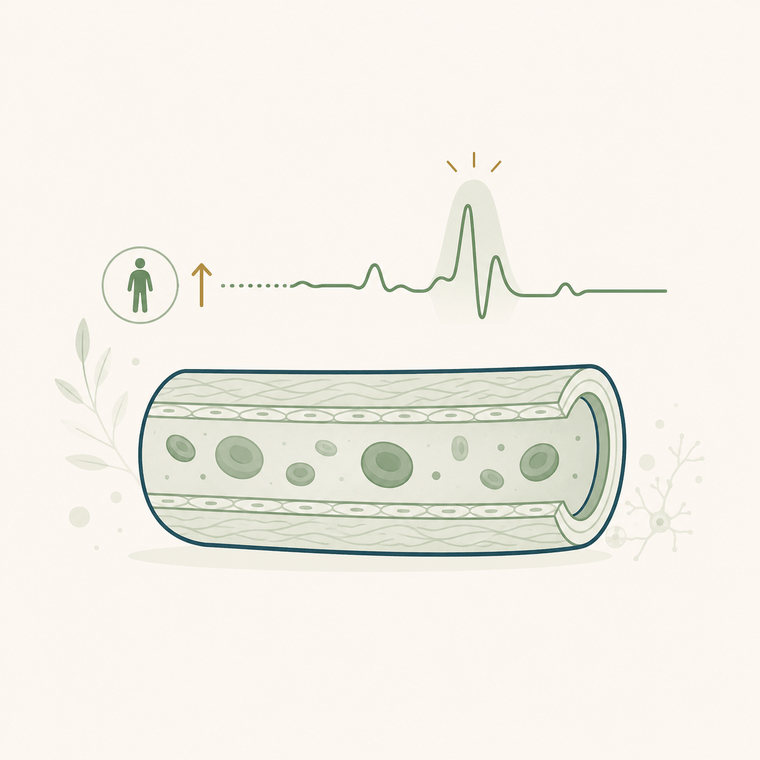
Heart & vessels
The inner lining of the vessels (endothelium) and the automatic circulatory regulation can be disturbed – hence palpitations on standing or dizziness (POTS).
What does this mean for me? Explains palpitations, dizziness and circulatory problems when standing.
Related symptoms: POTS · palpitations · dizziness
When inflammation and autoimmune reactions play a role
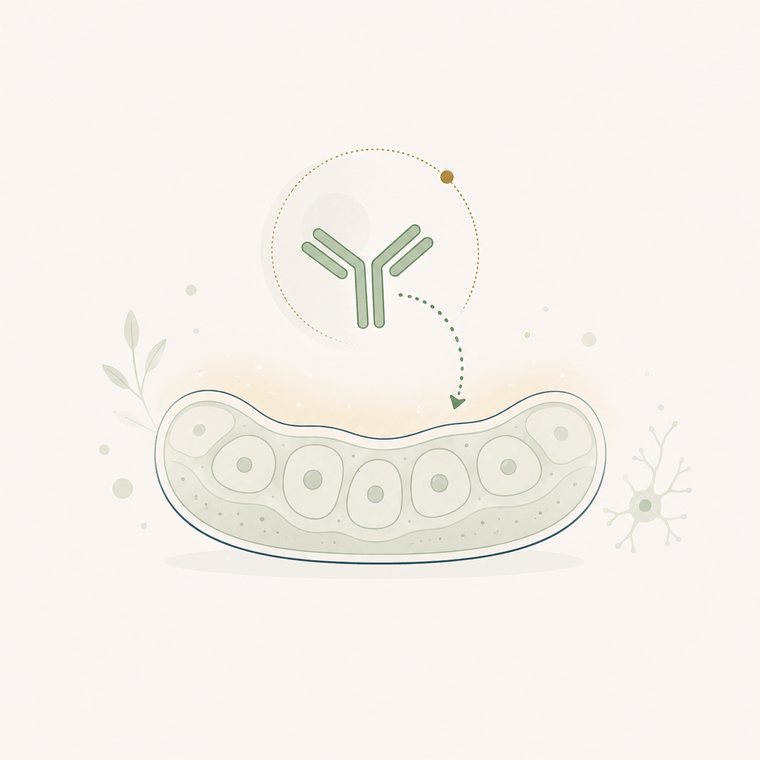
Inflammation & autoimmunity
Normally inflammation switches off again. In Long COVID it can persist; in part the immune system reacts to the body's own structures (autoantibodies).
What does this mean for me? Explains pain and a persistent 'inflamed' feeling.
Related symptoms: Pain · flare-ups · inflamed feeling
When energy supply and blood sugar may be connected
Glucose & insulin
The regulation of blood sugar and insulin can be altered after COVID (studies show an increased diabetes risk) – this affects how stable your energy is across the day.
What does this mean for me? Explains strong energy swings across the day.
Related symptoms: Energy swings · fatigue
POTS: why your pulse shoots up when you stand
In orthostatic intolerance (e.g. POTS), the autonomic nervous system regulates circulation less well on a change of position — lying down the pulse is calm, on standing it rises sharply, often with dizziness.
Schematic. Always have palpitations/dizziness on standing checked medically before changing anything.
How well is this proven?
Honest classification instead of promises of a cure. We use a five-level scale for how robust a statement is — and we say clearly what is still a hypothesis.
- 1No robust evidencespeculation, anecdotes or no credible basis of benefit
- 2Early signalsmall pilot studies or inconsistent results
- 3Moderate signalfirst human studies, but not yet conclusive
- 4Stronger evidenceseveral well-designed studies with consistent benefit
- 5Very strong evidencerobust, reproducible evidence at a high level
- Immune responseCombinatorial study
- Inflammation & autoimmunityCombinatorial study
- Cellular energy (PEM)Association/cohort data
- Heart & vessels (POTS)Association/cohort data
- Cognition / Brain FogHypothesis / biological plausibility
- Glucose & insulinHypothesis / biological plausibility
Clinical studies and reported everyday experiences are not the same.
Surveys like TreatME gather experiences from people with ME/CFS and Long COVID. Such data can give important hints — but they do not replace a controlled clinical efficacy test. We show both, but never as the same thing.
We build the outcome evidence transparently — together with clinical partners and anonymised. Until then we honestly show above what is proven and what remains a hypothesis.
Classification based on PrecisionLife and the combinatorial Long COVID/ME-CFS genetics. Genetic predisposition is not destiny — it changes probabilities, not certainties.
How your test is mapped onto this
Your test gives you no yes/no, but shows which of these six patterns are more pronounced in you than in other affected people – as orientation, not as a diagnosis. 'Associated' does not mean 'caused'.
- Genetic predisposition (fixed)
- Current state (changeable)
From your saliva, CeGaT reads your genotype profile (in Germany). The combinatorial PrecisionLife analysis (appliance on German servers) derives your percentile per mechanism from it. Important: your predisposition (dotted, fixed) is different from your current state (filled, changeable). The report shows both — and where sensible levers apply.
Illustrative example – no real personal data, not a diagnosis. Your data does not leave Germany.
Technical terms, simply explained
So nothing overwhelms you — the key terms in one sentence each.
An accredited German specialist lab that reads (sequences) your genome from your saliva sample.
The analysis method that detects combinations of many gene variants — running as a software appliance on servers in Germany.
Reading your DNA — like transcribing a very long text, letter by letter.
Your position compared to others. Percentile 80 means: this pattern is more pronounced in you than in 80% of the comparison group.
Your genotype is your personal gene pattern; imputation computationally fills in missing spots based on known patterns — standard in genetics.
Your report is not a PDF in a drawer
Long COVID fluctuates. That's why the report is a living document: your profile is re-measured at intervals so you can see change — and so we build outcome data together, instead of just promising it.
- Start
- after 4 weeks
- after 12 weeks
In the example, the pronounced patterns become calmer over weeks. This shows whether the jointly chosen levers are working — honestly, even when little changes.
Illustrative course, no real personal data and no promise of effect. You set the pace and goals with your doctor — PEM-safe, without performance pressure.
What you can concretely do after the report
A result is only useful when it's clear what comes next.
A high percentile means: this pattern is more pronounced in you — worth attention here. A low percentile is not 'bad luck': it just means this mechanism is less in the foreground for you — then other levers matter more. There are sensible, PEM-safe steps for everyone.
A made-up sample profile. Your real report shows your own values — the steps work the same way. A higher percentile means: this is where attention pays off first.
Strict pacing: stay 20–30 % below your limit, fixed rest windows — never force through exhaustion.
Take infections seriously early, recover generously; have notable values (e.g. iron, vitamin D) checked by your doctor.
Stand up slowly, more fluids and salt (agreed with your doctor), try compression stockings.
Reduce stimuli, one task at a time, deliberately schedule cognitive breaks.
No acute focus — keep sleep, recovery and low-stimulus routines stable as your base.
No acute focus — regular, simple meals are enough; no special measures needed.
Illustrative example, no real data, no diagnosis and no promise of effect — all steps are meant to be PEM-safe and should be discussed with your doctor.
- 1Download the summary for your doctor's appointment (below) and take it to your next visit.
- 2Start with pacing: activity below your limit, breaks before exhaustion — never force it.
- 3Use the tracker for 1–2 weeks to spot patterns and delayed worsening (PEM).
- 4Pick ONE lever from your strongest mechanism and try it gently — observe what changes.
Strict pacing + fixed rest windows; have iron/vitamin D checked medically.
Stand up slowly, more fluids/salt (coordinated with your doctor), compression; have palpitations checked.
Levers still apply: sleep hygiene, reducing stimuli, gentle energy management; track the course.
Illustrative examples, no real personal data and no promise of effect — coordinate everything with your doctor.
Summary for your doctor
Take this page to your next appointment. It summarises the matter factually — as a conversation aid, not a diagnosis.
- ·Subject: genetic orientation report (longcovid.expert) for Long COVID / ME-CFS — medically supervised, not a diagnosis.
- ·Method: CeGaT low-pass WGS (Germany) + combinatorial PrecisionLife analysis (appliance in DE, pseudonymous).
- ·Result: percentile profile across six mechanisms (immune, energy/PEM, cognition, heart/vessels, inflammation, glucose).
- ·My most pronounced mechanisms: ____________________ (fill in from the report).
- ·Context: associated is not the same as caused — genetic patterns are context, not a diagnosis or treatment decision.
- ·PEM note: please no graded exercise (GET) without consultation; pacing and exertion management first.
- ·My questions: ____________________________________________
Not a substitute for diagnosis. Data processing in Germany (GDPR Art. 9). For acute symptoms: emergency 112.
What you can do depending on your result — with medical guidance
If a mechanism is high for you, that is where attention pays off first. Below are PEM-safe self-help steps and — honestly graded by evidence — supplements that have been studied, each with a source.
No treatment recommendation, no diagnosis, no promise of cure. Genetic predisposition is not the same as your current state. Supplements can have side effects and interact with medication; some are unsuitable in certain conditions. Take nothing without medical clarification (incl. blood values) — we deliberately give no dosages. The underlying genetic analysis is a research signal (preprint).
→ Pacing first, fixed rest windows, stay below your limit — never force it.
With your doctor, check blood values (ferritin, B12, vitamin D, thyroid). Studied: coenzyme Q10 + NADH, plus B vitamins and magnesium — evidence limited.
No graded exercise therapy (GET) with PEM.
Show sources (2)
- Castro-Marrero et al. 2021 · RCT: CoQ10 (200 mg) + NADH (20 mg) over 12 weeks reduced cognitive fatigue and improved quality of life in 207 ME/CFS patients. DOI
- Mantle et al. 2024 · review: Overview of mitochondrial dysfunction and CoQ10 in post-viral fatigue syndrome (ME/CFS, fibromyalgia, long COVID) — promising, but no approved therapy yet. DOI
→ Reduce stimuli, one task at a time, cognitive breaks, prioritise sleep.
Have B12/folate checked if deficient; omega-3 and B vitamins are discussed for fatigue/cognition. There is little solid evidence for nootropics.
If deficiency is suspected, blood values first, then decide with your doctor.
Show sources (1)
- Tardy et al. 2020 · review: Review of the role of B vitamins, vitamin C, iron, magnesium and zinc in energy, fatigue and cognition — a deficiency can contribute to tiredness and cognitive symptoms. DOI
→ Stand up slowly, more fluids and salt, compression stockings, elevate your legs.
For POTS the first steps are mainly clinical (fluids/salt agreed with your doctor, compression) — there are no specific supplements with good evidence here. Have iron status (ferritin) checked.
Have palpitations or dizziness assessed by a doctor.
→ Take infections seriously early, recover generously, keep stimuli low.
Have your vitamin D status checked and corrected medically if low. Better avoid „immune boosters“ — they can harm if you have an autoimmune tendency.
No self-experiments with immune-stimulating agents.
Show sources (1)
- Matangkha et al. 2025 · association: Observational study (170 patients): lower vitamin D levels were associated with long COVID symptoms — a correlation, not proof of effect. DOI
→ Keep sleep, low stimuli and stress regulation stable as your base.
Omega-3 fatty acids are discussed as inflammation-modulating. Notable autoimmune signs belong in medical (rheumatology) assessment — do not self-treat.
Caution with „immune-strengthening“ agents in autoimmunity.
Show sources (2)
- Jiao et al. 2022 · review: Systematic review in lupus (SLE): omega-3 reduced inflammatory markers (ESR, CRP) and disease activity — from a related autoimmune context. DOI
- Livieratos et al. 2024 · review: Scoping review of long COVID therapies: omega-3 among others is being studied; overall, large robust trials are still lacking. DOI
→ Regular, simple meals, fibre, gentle movement within your exertion limit.
Have HbA1c checked medically. Magnesium is discussed in relation to metabolism and fatigue. (Metformin is being studied in long COVID trials — a prescription medication, not a supplement.)
No crash diets; manage metabolism with your doctor.
Show sources (1)
- Rodríguez-Morán et al. 2024 · RCT: Open-label RCT (60 long COVID patients with magnesium and vitamin D deficiency): magnesium chloride + vitamin D improved depressive symptoms more than vitamin D alone. DOI
Sources via PubMed, linked as DOI. Much is preliminary or comes from related conditions (ME/CFS, fibromyalgia, lupus) — not proof for your individual case. Take these points to your doctor's appointment.
Understanding PEM & crashes
PEM (Post-Exertional Malaise) is more than normal tiredness: symptoms worsen markedly after exertion — often only hours later or the next day. The most important protection is pacing (staying within your own energy limits), not pushing through. If PEM is suspected: no blanket exercise programme and no 'more movement helps' without medical consultation.
Pacing: staying under your energy limit
Schematically: staying within your own energy limit keeps things steady. Repeatedly going over it risks the typical boom-bust — a brief high, then a crash (PEM) that can cost days.
Schematic illustration, not measured data. Your personal limit is individual — explore it carefully and with medical guidance.
When a crash happens
A crash (PEM) can come with a delay — often only hours later or the next day. In such a situation, protection from stimuli and recovery help, not pushing through.
- 1Stop activity and reduce stimuli (dim the light, turn off sounds and screens).
- 2Get into a calm, comfortable position and rest.
- 3Have fluids ready — as is tolerable for you.
- 4Don't plan new exertion; postpone appointments if possible.
- 5Be patient with yourself — a crash is not a setback 'through your own fault'.
Acute warning signs: With new severe chest pain, severe shortness of breath or loss of consciousness, call emergency services (112) immediately.
General, PEM-safe orientation — not a substitute for medical advice.
What you can do with this knowledge — safely
Knowledge only becomes useful when it leads to a next step. For each mechanism one everyday-friendly lever — and a clear safety guardrail. No therapy, no promise of a cure; orientation that you place in context with your doctor.
Predisposition is not destiny
Your genes set a tendency — but they don't fix the outcome. Modifiable factors shift where you land. That's why the result is a corridor, not a fixed point.
sets a tendency — does not change
- ✓Pacing & energy management
- ✓Sleep & recovery
- ✓Stimulus & stress regulation
- ✓medically guided options
a corridor, not a fixed point
Lever: Pacing: dose activity below your limit, plan breaks before exhaustion sets in.
Safety: No 'more movement helps': graded exercise therapy (GET) can harm in PEM. When in doubt, less.
Lever: Split cognitive tasks into short blocks, reduce stimuli, set fixed recovery breaks.
Safety: Brain Fog is real, not a question of discipline. Don't 'push through' exertion.
Lever: Stand up slowly, drink enough, possibly more salt/compression — coordinate with your doctor.
Safety: Always have palpitations/dizziness checked medically before you change anything.
Lever: Plan for flare-ups in advance, consistently avoid overload during flare phases.
Safety: Flare-ups are not setbacks 'through your own fault' — recovery takes priority.
Lever: Keep a pain/flare diary, recognise personal triggers and relieve them deliberately.
Safety: Persistent pain/signs of inflammation belong in medical treatment.
Lever: Regular, stable meals — distribute energy evenly across the day instead of spikes.
Safety: No diet experiments on your own; if anything stands out, have blood sugar checked medically.
General, PEM-safe notes — explicitly not a substitute for medical advice or treatment. For Long COVID / ME-CFS: never force exertion.
Long COVID and ME/CFS
Long COVID and ME/CFS are overlapping, but not the same. Some affected people meet the ME/CFS criteria — PEM is then central. Classification belongs in medical hands; this hub does not replace a diagnosis or self-diagnosis, but prepares a good conversation.
Post-Exertional Malaise — marked worsening after physical, cognitive, emotional or sensory exertion, often delayed.
Myalgic Encephalomyelitis / Chronic Fatigue Syndrome — a severe chronic illness in which PEM is central.
A disorder of the autonomic nervous system, which automatically regulates circulation, pulse and digestion, among others.
Postural Tachycardia Syndrome — a strong rise in pulse and symptoms when standing up or standing for longer.
Symptom & activity tracker
A short daily tracker helps to recognise patterns — especially a delayed worsening after exertion. It is voluntary, local and printable.
Observe patterns without overwhelming yourself
A few entries are enough. The tracker should relieve you and not become an extra task — especially useful for recognising a delayed worsening after exertion (PEM).
Mockup note: entries stay only locally in the open browser — nothing is saved or sent. The tracker does not replace medical assessment.
Mini self-check
In six short questions you'll see which of the six mechanisms are currently in the foreground for you — as non-binding orientation. Takes under a minute; you can stop anytime.
1.I often feel as if I have an infection (fluish, ill), even without having a cold.
2.After exertion — often only hours or days later — a clear crash follows (PEM).
3.Concentration, memory or word-finding are hard for me ('Brain Fog').
4.When standing up or standing for longer I get palpitations or dizziness.
5.I have persistent pain or an 'inflamed' feeling in the body.
6.My energy fluctuates strongly with eating or across the day.
Which pattern dominates in you?
The medically supervised report maps your genetic patterns onto exactly these six mechanisms. Calmly explained, with sources – not a diagnosis, not a promise of a cure.
Sources incl.: PrecisionLife (Long COVID & ME/CFS) · Smedley/Taylor/Sardell et al. (combinatorial genetics, J Transl Med 2023–2026) · WHO Post-COVID-19 Condition · CDC Long COVID/ME-CFS · gesund.bund.de · NICE NG206/NG188. Educational — does not replace medical advice; for acute symptoms call 112.